This post is part of a series about my brother’s upcoming book Addiction Nation: What the Opioid Crisis Reveals about Us, discussing some of the science and stats he used throughout the books. Read the intro post here, part 1 here, part 2 here, part 3 here, or (best of all) pre-order the book on Amazon here. Only 2 more days until the release!
We’ve spent the last few weeks looking at a lot of areas of addiction, but (much like your book) I wanted to end this series on a positive note….talking about recovery and hope. Of course one of the biggest reasons people want to read about addiction is precisely to find hope, so I think it’s a good place to end. Sound good?
Tim: Awesome! I wanted to note one other hopeful thing up front. There are some pretty terrible treatment programs out there. I didn’t get into the corruption or the number of facilities that don’t use evidence-based treatment methodologies. They really do have low success rates.
One critical thing to look at is how specific studies define “success.” If they only definition of “success” is total abstinence for a person’s entire life (or even just the length of the study) then a lot of numbers are going to look pretty grim. But, if success is defined by decreasing overdoses, a reduction in harmful behavior or even just using less of the substance, then there is a lot of reason to hope.
Another thing I didn’t get to dive into is “spontaneous remission” or when a person recovers from an addiction without any professional treatment. It happens a lot more than you would expect. This means that increasing access to treatment is really important but we can also save a lot of lives by trying to keep people alive long enough for that spontaneous remission to occur.
Ooooh….defining success metrics clearly. I like it.
Okay, so first up, last week we talked about the Rat Park study, and you mentioned a study that often gets brought up with that one. It’s a 1974 study called “How Permanent Was Vietnam Drug Addiction?“, and it looked at the rates of addiction among American soldiers in Vietnam as they were leaving Vietnam, then got back in touch with them after they got home. The results are here:

The most often quoted statistic (and the one you use in the book) is the amazing drop from 20% reporting an addiction issue to just 1% reporting an issue a year later. It’s an incredible statistic, made stronger by the fact that this study had a very low non-response rate (<5%) and that urine testing backed up the self reported usage. You quote the study as saying:
There have been no studies of addict populations in this country that show anything like the 95 percent remission rate after ten months, which is what a drop from 20 percent addicted while in Vietnam to 1 percent after Vietnam suggests.
I can see why that stat gets all the headlines, but one of the things I found most interesting about this study when I dove in to it was that there’s actually a lot more in it for us to think about. You weren’t able to get in to it in the book, but I found their breakdown of the subgroups within that group fascinating:
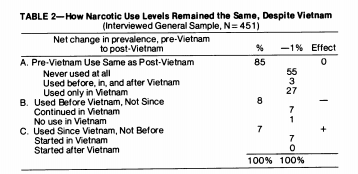
So basically 85% of soldiers returned to their pre-Vietnam status. 8% who had used before Vietnam actually stopped using after returning from Vietnam, and 7% who weren’t using before started using and never stopped.
Now the authors throw in a caveat here that just because these veterans stopped using narcotics doesn’t mean they didn’t pick up another problem (alcoholism, barbiturates, etc), and they note that those who continued their addiction tended to have a much bigger problem than they did before going to Vietnam. However, even with those notes, this does fly in the face of the idea that using narcotics will always lead to a permanent addiction problem with that particular substance.
Tim: Absolutely. There is a good reason to believe that this is the norm, not the exception. This is why “heroin-assisted treatment” has been pretty well documented to be effective in the long term. It reduces other health risks, like Hep C and HIV, provides consistent dosage and reduces drug-related crimes. While some people will just keep using indefinitely, a lot of others will experience spontaneous remission or eventually decide to engage in another kind of treatment.
It also indicates that there are almost certainly people who might be more “situational” addicts, and we may need to treat them differently from those whose addictions seem more persistent. Looking at your story, one could call you a “situational” addict, don’t you think? Any thoughts on this?
Tim: The Vietnam study was actually the inspiration for Bruce Alexander’s “Rat Park.” I think Alexander would argue that almost everyone is a “situational” in their addictions.
I wouldn’t want to create a strict duality but think this a better category for a spectrum, how big a role does your situation play? For alcohol consumption, there are a lot of folks who have problematic consumption levels that could be classified as alcoholism throughout college and into their twenties and early thirties. But, they eventually change their behavior in a way that is often triggered by major life events.
But, in Switzerland, about 20% of people have continued using since the beginning of the heroin-assisted treatment program. This remaining population would probably be covered by life trauma, mental illness and some other genetic factors.
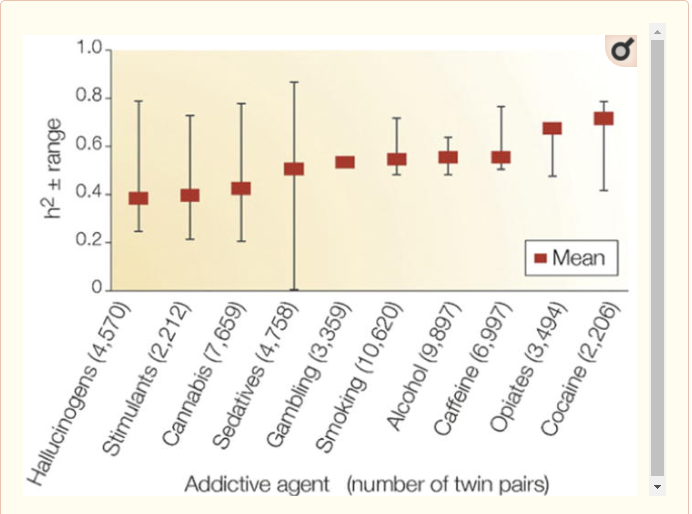
While I focus a lot on environmental and social factors for addiction, you can’t escape some sort of genetic predisposition. Even if it isn’t necessarily for “addiction” but a bodily response to certain substances.
For example, both us were prescribed opiates in high school/college for oral surgery. You took them and felt terrible. As soon as you could, you moved to ibuprofen because the narcotics made you feel sick. I finished the entire bottle, even though my surgery was less significant because I really enjoyed how they made me feel.
That’s true. I get incredibly nauseous when I take opioids and have refused them ever since that surgery. Taking enough of them to get addicted would be a downright struggle for me.
Okay, to tease out one last part of that study, I found the entire idea that 8% of the men had a problem before they went to Vietnam but came back and stopped using totally fascinating. That’s pretty much the reverse of what we tend to think about with addiction….that traumatic events must always make it worse. With addiction though, we know this isn’t always the case. As you say in your book:
As discussed earlier, over time, severe addiction reduces the amount of gray matter in the part of our brain most responsible for higher-level reasoning and self-control. A 2013 study of the brains of those struggling with cocaine addiction suggests something interesting. Within a few months of sobriety, that gray matter began to return. Within six to twelve months, the gray matter had returned to baseline levels and was about the same as those who had never been addicted. But soon after that is when the most amazing thing happened: those areas began to form an even greater level of density than for those who had never used cocaine.
You got this from a study called “Dissociated Grey Matter Changes with Prolonged Addiction and Extended Abstinence in Cocaine Users“, which contained this very cool graphic:
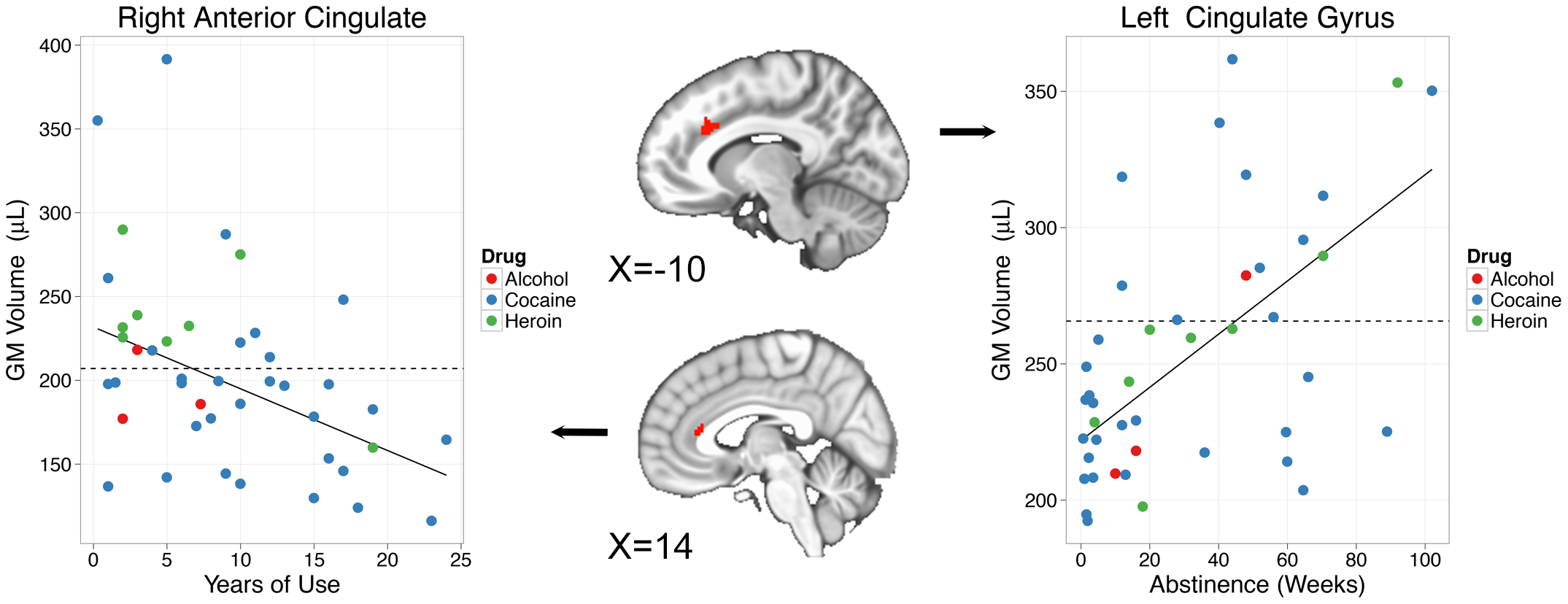
So basically, substance use can get bad in a hurry because many substances actually erode the very parts of the brain that normally help us avoid doing impulsive things. Prolonged abstinence actually reinforces those parts of the brain beyond the baseline levels. As the study says:
If addiction can be characterized as a loss of self-directed volitional control , abstinence and its maintenance may be characterized by a reassertion of these aspects of executive function. Current cocaine users demonstrate reduced GM in brain regions critical to executive function, such as the anterior cingulate, lateral prefrontal, orbitofrontal and insular cortices. In contrast, the group of abstinent CD users reported here show elevations in GM as a function of abstinence duration that exceeds control levels after 36 weeks, on average, of abstinence.
They do note (as all good studies do) that they don’t really know causality here either. It could be that these addicts had above-average levels of grey matter beforehand (they were not measured pre-addiction) or it could be that recovery caused them to grow more grey matter than they originally had. It could be a little of both. It’s pure anecdote, but based on what I’ve seen out of successful recovered addicts I’ve known, I’d say the change is real. How about you? On a personal level, do you feel addiction and recovery changed your brain at all?
Tim: My struggle would be classified as a relatively mild opioid use disorder. While the addictive process at work certainly would have changed my brain it would have been less significant than if it had gone on for years or decades. Since the initial change was not as substantial I don’t think my process of recovery likely changed things as much.
I have been amazed that whenever I talk with someone who is also open about their recovery, there is often a sense of connection because there are different truths we’ve realized about ourselves that creates a kind of bond.
Three thoughts related to that.
First, I wanted to tell my story because early detection matters. If you are able to see what is happening and get support early on, recovery won’t be as difficult. I think a lot of people end up letting an addiction progress because of the shame and stigma that surrounds it. Admitting you are feeling out of control seems like a life and world ending admission. That makes it harder to do.
Second, I do think this journey has led me to a place of diving deeper into the techniques of cognitive behavioral therapy. My research in that area made me realize how important those tools can be for improving my outlook and life more broadly. Writing a book about opioid addiction made me reflect on my alcohol consumption. It isn’t problematic at the moment but if I was to continue to drink 1-2 more alcoholic beverages a week for the next 10-20 years, there could be significant negative effects. So, I’ve started using what I’ve learned to be more thoughtful about the role alcohol plays in my life.
Third, has been a deepening of my own spiritual and religious practices including various forms of meditation and prayer. Mindfulness training is now integrated into a lot of different recovery practices. Even though I don’t feel a day to day tug towards opioid usage, I’ve tried to dig into these practices that could provide some anchoring because I am now well aware how easily the addictive process can kick up.
Alright, well that wraps up the series! If you want to see more from my brother, take a look at his book/author page here or buy the book and get it on Tuesday! Anything else you want to say to the nice people Tim?
Thanks for reading and I’m sure I’ll be back some time soon!
Agreed! You didn’t put it in the book, but I’d love to dig more in to the research around some of the heroin assistance programs. Crazy stuff.
Thanks for posting brother, and thank you so much for letting me opine on your work. It’s been an honor to go through so much of this journey with you, both the addiction part and the book writing part. I’m proud of you on both counts, and can’t wait to see what’s next in your journey.