Well hello again! Apparently I’m just falling behind all over the place with this. An update a month was a nice aspiration, but not one I’m managing. Moving on! Last time I posted we were just under 1.1 million excess deaths since 2/1/20, and as of 6/1, we are at 1.125 million. That actually seems….pretty good comparatively? I only have the numbers from 6/1 because the CDC is doing some sort of work on their database and won’t have updated numbers until next week. We’ll see when I get around to looking at those.
Alright, on with what we have!
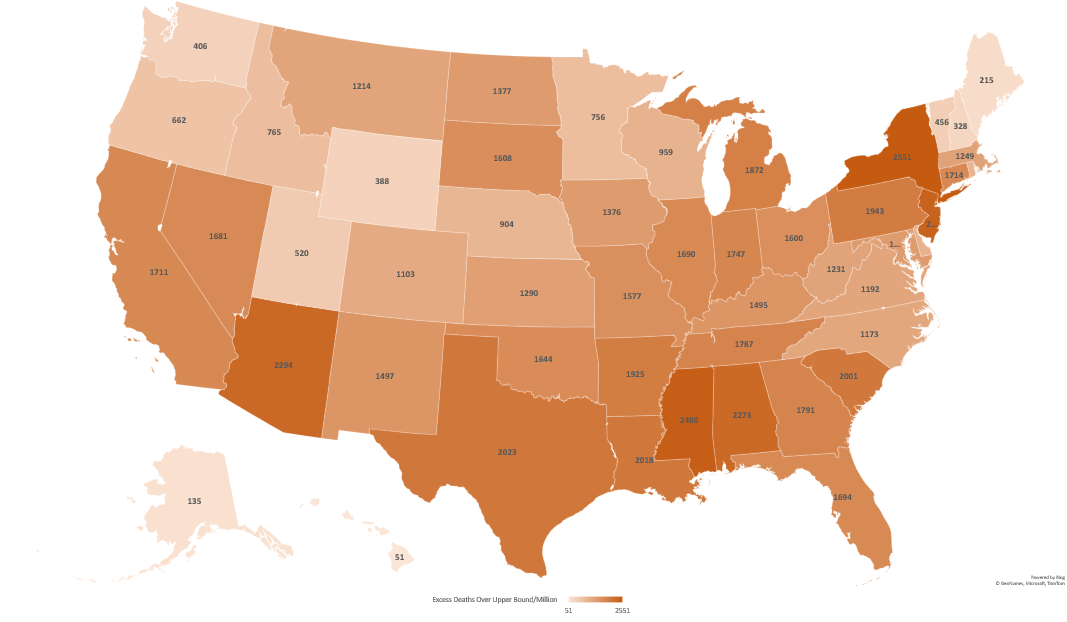
Excess Mortality Above Average
First up, the map. When I posted on 3/23, the range at the bottom was 1020-5729 deaths/million residents. Now it’s 1047-5823 deaths/million. For a 10 week gap that is….not a bad change. Certainly better than we’ve seen since I’ve been doing this. So where are the bad states?

| State | Excess Deaths Above Average 2/1/20-6/1/22 | Change from 3/23/22 | Change in Rank |
|---|---|---|---|
| Mississippi | 5823 | +94 | No change |
| West Virginia | 5622 | +912 | +2 |
| Arizona | 5153 | +205 | +1 |
| New Mexico | 4848 | +206 | +1 |
| Alabama | 4841 | +73 | -2 |
| Louisiana | 4506 | +237 | +2 |
| Tennessee | 4480 | +80 | +1 |
| Arkansas | 4467 | +104 | -1 |
| Wyoming | 4353 | +186 | +2 |
| South Carolina | 4287 | +85 | -1 |
Wow…so that was a jump. They jumped last time as well, so they are moving quite rapidly. What other big movers were there?
| State | 6/1/22 Excess | 3/23/22 Excess | Change | June Rank | March Rank |
|---|---|---|---|---|---|
| West Virginia | 5622 | 4710 | 912 | 2 | 4 |
| North Carolina | 3369 | 2556 | 813 | 24 | 42 |
| Puerto Rico | 1972 | 1407 | 565 | 48 | 51 |
| Alaska | 3208 | 2927 | 281 | 28 | 34 |
| Louisiana | 4506 | 4269 | 237 | 6 | 8 |
| New Mexico | 4848 | 4642 | 206 | 4 | 5 |
| Arizona | 5153 | 4948 | 205 | 3 | 2 |
| Oklahoma | 4267 | 4077 | 190 | 11 | 12 |
| Wyoming | 4353 | 4167 | 186 | 9 | 11 |
| Kentucky | 4155 | 3971 | 184 | 13 | 13 |
Interesting, so West Virginia and North Carolina are our two big jumpers here. I’m not clear why that is, but it’s worth noting that North Carolina had been outperforming it’s neighbors for quite some time, and is still outperforming them now. Peurto Rico was also doing very well and it’s jump has it doing only slightly less well.
It’s also worth noting that 9 states lost excess deaths in the last 10 weeks. We had wondered if we were going to see this effect start to happen, as this is something that could occur if some of the people who died initially were those who were close to death already. These states were: Rhode Island (-205), Ohio (-72), Maryland (-62), New Jersey (-52), Massachusetts (-34), Michigan (-31), Illinois (-20), Idaho (-19) and Pennsylvania (-17).
It will be interesting to see if more states start to slip backward as the summer goes on.
Percent Excess Mortality – 2020 and 2021
Alright, so hopefully most states are done updating their numbers from 2020 and 2021 by this point right? Who’s still at it? Well, really only Alaska (+2%), North Carolina (+7%), North Dakota (+8%) and West Virginia (+4%). All other states have very small changes or no change in the last 10 weeks. Top 10 states for each year are highlighted and bolded below, though 2021 had a 3 way tie for 10th so there are actually 12 states there.
| State | 2020 deaths – expected | 2020 deaths – actual | % change | 2021 deaths – expected | 2021 deaths – actual | % change |
| Alabama | 54839 | 62550 | 14% | 55036 | 67508 | 23% |
| Alaska | 4462 | 4971 | 11% | 4552 | 6037 | 33% |
| Arizona | 62622 | 75955 | 21% | 63797 | 82520 | 29% |
| Arkansas | 33424 | 37432 | 12% | 33406 | 40015 | 20% |
| California | 284264 | 315430 | 11% | 275238 | 336534 | 22% |
| Colorado | 41621 | 47161 | 13% | 41289 | 48912 | 18% |
| Connecticut | 32416 | 37730 | 16% | 32910 | 34479 | 5% |
| Delaware | 10016 | 10862 | 8% | 10247 | 11295 | 10% |
| District of Columbia | 6959 | 7378 | 6% | 6495 | 7130 | 10% |
| Florida | 213923 | 240765 | 13% | 219931 | 264812 | 20% |
| Georgia | 87875 | 102464 | 17% | 89319 | 112573 | 26% |
| Hawaii | 11893 | 11990 | 1% | 12343 | 12839 | 4% |
| Idaho | 15138 | 16340 | 8% | 15282 | 18299 | 20% |
| Illinois | 108823 | 127440 | 17% | 108444 | 120592 | 11% |
| Indiana | 69474 | 78293 | 13% | 69171 | 79198 | 14% |
| Iowa | 30946 | 35418 | 14% | 31547 | 33809 | 7% |
| Kansas | 26882 | 30773 | 14% | 27392 | 30975 | 13% |
| Kentucky | 50994 | 55145 | 8% | 50136 | 60206 | 20% |
| Louisiana | 47208 | 56320 | 19% | 48057 | 57469 | 20% |
| Maine | 15070 | 15504 | 3% | 15347 | 17045 | 11% |
| Maryland | 53119 | 59048 | 11% | 53311 | 57396 | 8% |
| Massachusetts | 61009 | 68390 | 12% | 62383 | 63748 | 2% |
| Michigan | 98748 | 114510 | 16% | 100176 | 115524 | 15% |
| Minnesota | 46084 | 51732 | 12% | 47005 | 51225 | 9% |
| Mississippi | 32284 | 38825 | 20% | 32315 | 40348 | 25% |
| Missouri | 66643 | 75514 | 13% | 68207 | 76413 | 12% |
| Montana | 10651 | 11903 | 12% | 10400 | 12771 | 23% |
| Nebraska | 17173 | 19547 | 14% | 17863 | 19052 | 7% |
| Nevada | 28547 | 31006 | 9% | 27546 | 33974 | 23% |
| New Hampshire | 13127 | 13435 | 2% | 13464 | 13775 | 2% |
| New Jersey | 76686 | 94621 | 23% | 78694 | 83497 | 6% |
| New Mexico | 19180 | 22842 | 19% | 19616 | 24433 | 25% |
| New York | 101705 | 118274 | 16% | 103179 | 115838 | 12% |
| New York City | 54870 | 81660 | 49% | 55622 | 63259 | 14% |
| North Carolina | 99977 | 108916 | 9% | 100298 | 118893 | 19% |
| North Dakota | 7233 | 8793 | 22% | 7508 | 8065 | 7% |
| Ohio | 130487 | 142211 | 9% | 130056 | 147109 | 13% |
| Oklahoma | 40731 | 45814 | 12% | 41086 | 49214 | 20% |
| Oregon | 37707 | 39947 | 6% | 37171 | 44825 | 21% |
| Pennsylvania | 140989 | 154622 | 10% | 139294 | 156273 | 12% |
| Puerto Rico | 30574 | 32056 | 5% | 30695 | 33090 | 8% |
| Rhode Island | 10399 | 12054 | 16% | 10877 | 11598 | 7% |
| South Carolina | 51380 | 59676 | 16% | 52784 | 64260 | 22% |
| South Dakota | 8456 | 10052 | 19% | 8447 | 9362 | 11% |
| Tennessee | 78370 | 87418 | 12% | 78956 | 95155 | 21% |
| Texas | 212670 | 250917 | 18% | 214835 | 271773 | 27% |
| United States | 2956302 | 3353789 | 13% | 2958796 | 3468553 | 17% |
| Utah | 20042 | 22027 | 10% | 20069 | 23454 | 17% |
| Vermont | 5853 | 6116 | 4% | 5791 | 6617 | 14% |
| Virginia | 71636 | 78680 | 10% | 72781 | 84878 | 17% |
| Washington | 59364 | 62558 | 5% | 59889 | 68415 | 14% |
| West Virginia | 23033 | 25323 | 10% | 23605 | 28679 | 21% |
| Wisconsin | 54583 | 61940 | 13% | 55622 | 60532 | 9% |
| Wyoming | 4324 | 5497 | 27% | 4867 | 5951 | 22% |
So there we go! The good news is things actually do look to be finally slowing down quite substantially in most places. A few states still look to be struggling, though at this point it’s unclear what’s driving that.
As always, add any questions in the comments or shoot me a message!